Real-Time Biological Measurement for Sepsis Treatment Decisions
Legacy microbiology infrastructure scales through larger instruments, centralized workflows, and operational complexity.
Guanine scales through programmable signal density, computational measurement, and compact electrochemical systems. A programmable signal architecture enables functional susceptibility, pathogen identification, and dynamic biological response measurement within the clinical decision window.
Advanced biological measurement becomes deployable:
- outside centralized labs
- closer to treatment decisions
- at substantially lower system cost
Sepsis Treatment Decisions Occur Before Biology Becomes Measurable
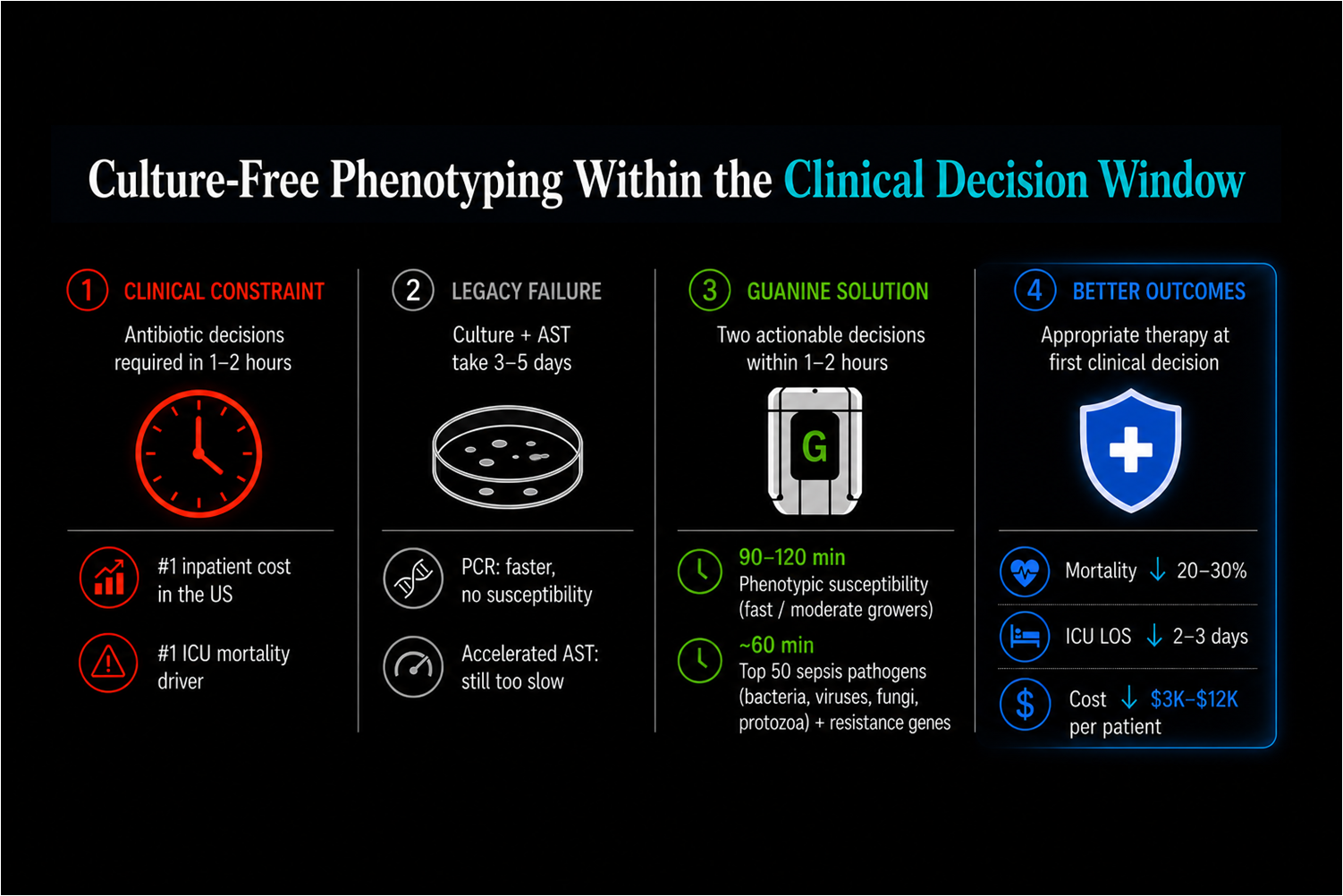
Sepsis treatment decisions occur within 1–2 hours, while conventional microbiology systems require sequential growth-dependent workflows operating over days.
As a result, the most important treatment decisions occur before definitive biological information exists.
Earlier functional therapy selection can reduce:
- mortality
- ICU length of stay
- empirical escalation
The clinical value emerges because biology becomes measurable early enough to alter treatment behavior.
Culture remains clinically valuable because it measures functional susceptibility. The limitation is not biological validity. The limitation is timing.

Conventional Microbiology Systems Cannot Operate Within the Clinical Decision Window
Traditional microbiology systems depend on organism isolation, amplification, and endpoint growth detection before functional susceptibility becomes measurable.
Faster molecular systems improve identification timing but remain disconnected from measured treatment response.
The problem is architectural fragmentation:
- pathogen identity
- susceptibility
- host response
- treatment monitoring
all operate in separate workflows with incompatible timing.
Functional Susceptibility and Pathogen Identity Within One Signal Architecture
Guanine collapses pathogen detection, susceptibility measurement, and dynamic biological monitoring into a unified electrochemical signal architecture.
Instead of waiting for endpoint culture growth, biological response becomes continuously measurable through programmable signal generation, multiplex encoding, and waveform stabilization.
This enables:
- rapid pathogen identification
- culture-free phenotyping
- time-resolved susceptibility monitoring
- quantitative biological response measurement
within the same clinical decision window.


Measuring Biological Response Directly Instead of Waiting for Growth
Conventional AST infers susceptibility from delayed organism growth. Guanine measures biological response dynamically under antibiotic exposure in real time.
Electrochemical response trajectories diverge continuously across susceptible, intermediate, and resistant states, enabling functional classification within 90–120 minutes for fast and moderate doublers.
Rather than accelerating culture workflows, the architecture bypasses growth-dependent timing entirely.
Rapid Measurements for Sepsis Management
Instead of fragmented workflows separated across laboratories and days, biological information becomes time-aligned to clinical intervention.
This creates a closed-loop biological decision system operating within the initial treatment window.

Sepsis Is the First Application of Real-Time Biological Measurement
Guanine is not accelerating conventional microbiology workflows.
It is introducing a programmable biological measurement architecture capable of transforming how dynamic biological systems are measured, interpreted, and acted upon in clinical environments.
Sepsis becomes the first large-scale deployment of real-time clinical biology.
Sepsis Diagnosis at the Speed of Clinical Decision
Time-aligned diagnostics delivering actionable insight across the first critical hours of sepsis—plus upcoming product configurations.